

Women’s Health Survey, all ages of women are affected, how are you?
Women are more likely to speak to family and friends, ask Google or do online searches than seek out a GPs help, data from


In 2021, it was reported that over 4 in 5 women (85%) have been comfortable talking to healthcare professionals about health concerns, with a rate of 3 in 5 women feeling comfortable talking to healthcare professionals about mental health conditions. The specific health conditions outlined with the most responses suggest that gynaecological conditions need more research and care from healthcare professionals.
Women’s Health Survey
The Women's Health Survey consisted of a publicly opened survey, available for all individuals aged 16 and over living in England. In March 2021, the Secretary of State for Health and Social Care and the Minister of State for Patient Safety, Suicide Prevention and, Mental Health launched a call for evidence seeking views on the first-ever government-led Women’s Health Strategy for England.

The responses varied among individuals, with some answering for themselves and others sharing their experiences of a female family member, friend, or partner. This also included the reflections of health and care professionals. Women aged between 30-39 years old responded at a higher rate than other age groups. Women aged between 30-39 years old responded at a higher rate than other age groups. They regarded their biggest concern as being gynaecological conditions. Women between the ages of 30-39 regarded their major issues of women's health as fertility, pregnancy, pregnancy loss, and post-natal support.
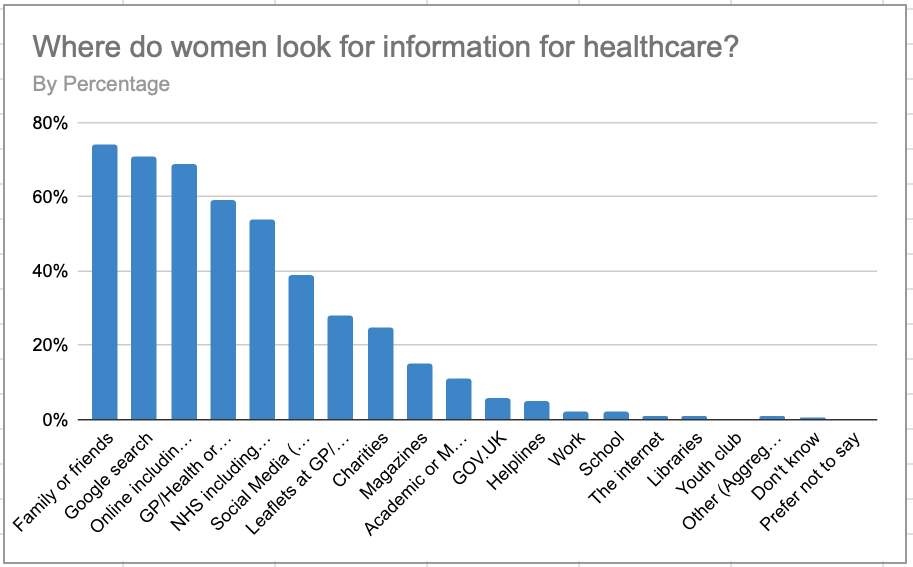
Data shows that women are most likely to ask family or friends for information about symptoms first, before the NHS.
Why are women not listened to when talking about symptoms and conditions to healthcare professionals?
Research shows that women feel ignored when seeking medical help. Gaslighting in the medical field has always been a prevalent issue, as Dr. Mieres from the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell says there is a ‘one size fits all approach to diagnosis and medicine’ which some doctors still follow, and in response, he is integrating sex and gender into the school’s curriculum. He argues that in recent decades, evidence has ‘emerged to show how sex and gender impact various diseases’, following on to say that healthcare delivery is behind the times.
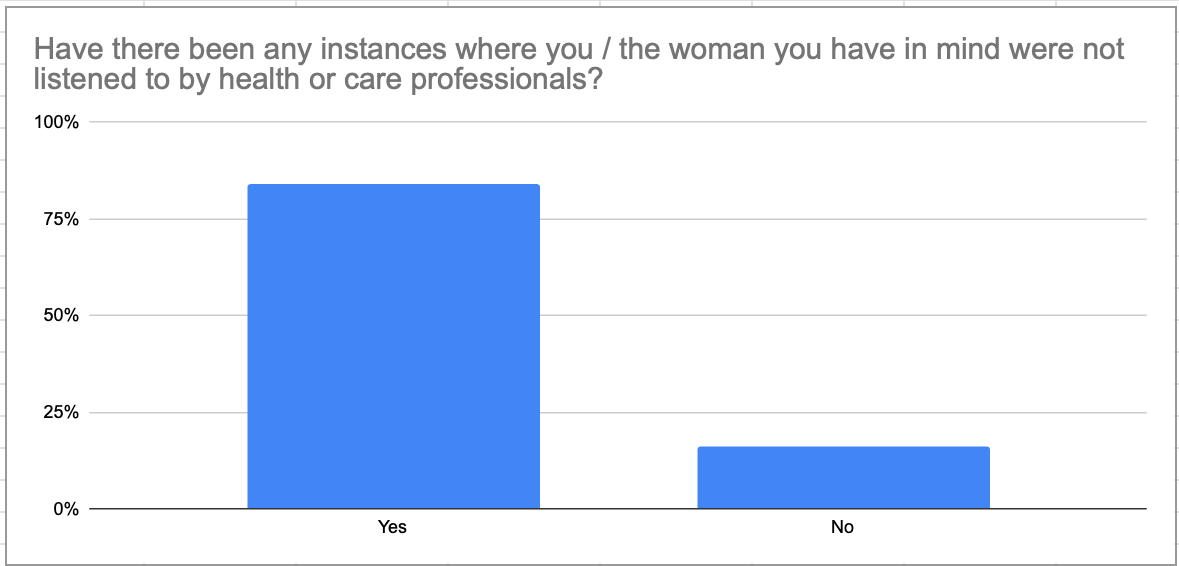
Female patients often experience dismissive attitudes from doctors, condescending remarks when notifying professionals about symptoms, and being told that the reason behind their ailment is because of hormones, stress, or ageing. These are just a handful of reasons why the responses from the survey showed that 4 in 5 women agreed they were not listened to by healthcare professionals.
If women are left feeling uncomfortable or unheard about their symptoms or conditions, this can lead to untreated and painful conditions, such as postnatal depression and fibroids. For example, fibroids, (a non-cancerous growth that grows around the womb) are most common in women ages 30-50 years old, and the symptoms are like those of common issues like menopause, periods or pregnancy, like abdomen and back pain, pain or discomfort during sex and, painful periods - leading to dismissal from GP’s and health professionals.
Another diagnosis such as Endometriosis presents a painfully long diagnosis wait, where the average individual is waiting around 8 years. Endometriosis can cause infertility and reproductive damage, affecting around 1 in 10 women in the UK.
Furthermore, the women’s health survey found that if women did secure a diagnosis, there were limited opportunities to ask questions about treatment options.

Sex-Education and it’s effectiveness
Currently, sex and health education - including the covering of menstruation, contraception, fertility, pregnancy, and menopause is now a statutory part of the school curriculum from 2020. This (although shockingly only recently made mandatory) means the current generation will learn about their bodies at school, in turn making women's health issues less of a stigmatised subject for years to come - meaning women will feel more comfortable discussing conditions and symptoms with healthcare professionals.
‘The goal of this 10-year strategy is to improve health experiences and outcomes for women, and includes a commitment to commission a Women’s Reproductive Health Survey every two years’ - Dr Rebecca French, Associate Professor of Sexual and Reproductive Health Research at the London School of Hygiene & Tropical Medicine.
Data from the survey
The data and evidence from the survey show that results of scientific research are not necessarily split by gender, invalidating any results due to the lack of study on differences between sexes. The research should be separated into: ages, racial backgrounds, and whether the women responding to the research have any pre-existing conditions or disabilities to give a fair representation of and to accurately identify where, how, and why the problem is occurring. The topic of health issues specific to women, such as gynaecological conditions and cancers, fertility, pregnancy, pregnancy loss and post-natal support, menopause, and menstrual health could be prioritised and offered research opportunities to guarantee diversity and support for women.
Data used in the article:
Further reading:
https://www.northwell.edu/katz-institute-for-womens-health/articles/gaslighting-in-womens-health